Falcon Pro
SUPPLYING THE WORLD’S LEADING PERIPHERAL VASCULAR DIAGNOSIS SYSTEMS
Falcon Pro
SUPPLYING THE WORLD’S LEADING PERIPHERAL VASCULAR DIAGNOSIS SYSTEMS
Vascular Solution

The FALCON Product line is a market leading peripheral vascular diagnosis system. The FALCON systems are an imperative for any vascular lab, large hospital or a private clinic. The FALCON/Pro is the most innovative, advanced and non-invasive peripheral vascular diagnostic system. Designed by Viasonix, it provides simple and efficient operation, offering a wide range of specialty tests.
Features
Advanced State-Of-The-Art Technology
- IPU technology provides reliability and high durability
- Ultimate configuration flexibility
- Full colour Doppler spectral display
- Simultaneous measurements for time effectiveness
- Camera connection for documenting pathologies
- Cybersecurity compliance
Unmatched User-Friendly Operation
- One Key Operation
- Designed for Touch Screen
- Unlimited Flexible Protocols
- Configurable Display Layout
- Colour Coded Tubes and Sensors
- Flexible Reporting Formats
- Language Support
Time Saving Options
- Automatic Examination Modes
- Auto-Inflate Option
- Auto-detection of systolic pressures
- Auto-Target Pressure
- Auto-Save for all measurements
SectionComplete Network Solution
- Practically Plug-and-Play DICOM operation
- DICOM (PACS) Worklist and Storage
- Programmable Structured Reporting
- HL7 Interface
- GDT Connectivity
- Unlimited Review Stations
- Shared network database via SQL
Ideal Research Solutions
- Variety of export formats including Raw Data
- PVR Analysis
- Built in statistics tool
- Informative charts and comparisons
- Data mining
The FALCON Product line is a market leading peripheral vascular diagnosis system. The FALCON systems are an imperative for any vascular lab, large hospital or a private clinic. The FALCON/Pro is the most innovative, advanced and non-invasive peripheral vascular diagnostic system. Designed by Viasonix, it provides simple and efficient operation, offering a wide range of specialty tests.
Features
Advanced State-Of-The-Art Technology
- IPU technology provides reliability and high durability
- Ultimate configuration flexibility
- Full colour Doppler spectral display
- Simultaneous measurements for time effectiveness
- Camera connection for documenting pathologies
- Cybersecurity compliance
Unmatched User-Friendly Operation
- One Key Operation
- Designed for Touch Screen
- Unlimited Flexible Protocols
- Configurable Display Layout
- Colour Coded Tubes and Sensors
- Flexible Reporting Formats
- Language Support
Time Saving Options
- Automatic Examination Modes
- Auto-Inflate Option
- Auto-detection of systolic pressures
- Auto-Target Pressure
- Auto-Save for all measurements
SectionComplete Network Solution
- Practically Plug-and-Play DICOM operation
- DICOM (PACS) Worklist and Storage
- Programmable Structured Reporting
- HL7 Interface
- GDT Connectivity
- Unlimited Review Stations
- Shared network database via SQL
Ideal Research Solutions
- Variety of export formats including Raw Data
- PVR Analysis
- Built in statistics tool
- Informative charts and comparisons
- Data mining
Segmental Blood Pressure
The Segmental Blood Pressure (SBP) tests require the placement of dedicated pressure cuffs on the various limb segments, which typically include the 2 brachial segments, the thighs (some protocols divide the thigh into 2 separate segments), the segment below the knees, the ankles and the toes.

Additional segments can be measured, such as the digits for diagnosis of the Raynaud’s Syndrome.
Prior to segmental cuff inflation, a reference signal is identified distal to the cuff location. This reference signal is typically a CW Doppler measurement or a PPG (Photo-Plethysmograph, used for the digits and toes).
When the cuff pressure exceeds the systolic pressure, the reference signal waveforms should disappear. Then, the cuff pressure is slowly deflated at constant bleeding rate, and the first occurrence, of the reference signal waveform return, marks the systolic pressure. The clinician is normally interested in the ratio of the ankle systolic pressure to the brachial pressure (ABI – Ankle Brachial Index), or in significant pressure differences either in sequential segments or side-to-side differences for the same segment.
Ankle Brachial Index (ABI)
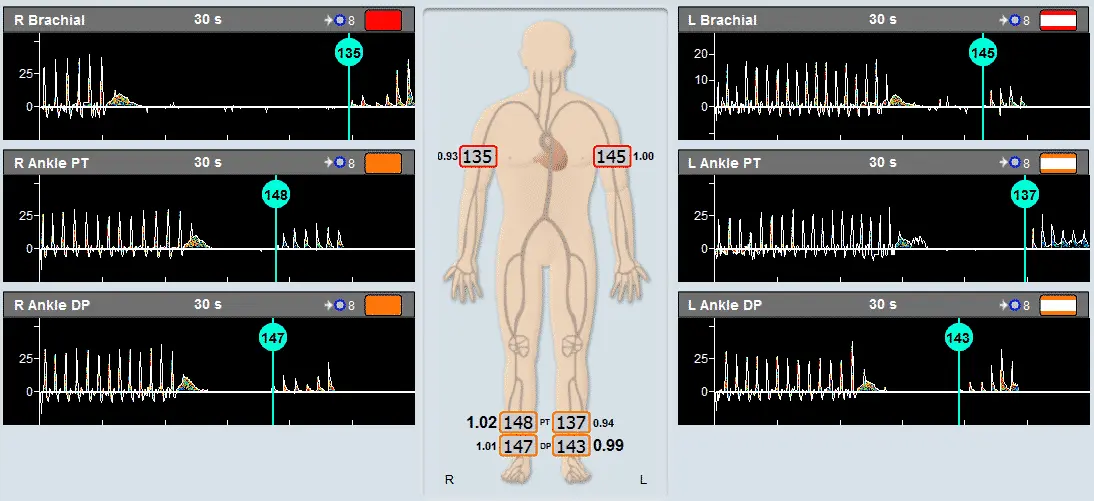
ABI, the Ankle Brachial Index, is the most popular application for fast and simple screening of a physiological vascular pathology. With this test pressure cuffs are placed on the 2 ankles and on 1 or 2 brachial segments.
The Viasonix FALCON Pro allows to perform the ABI test with either Doppler or PPG sensors. In addition, the Falcon allows to perform simultaneous measurements in all sites under certain conditions for rapid measurements.
Prior to segmental cuff inflation, a reference signal is identified distal to the cuff location. When the cuff pressure exceeds the systolic pressure, the reference signal waveforms should disappear. Then, the cuff pressure is slowly deflated at constant bleeding rate, and the first occurrence, of the reference signal waveform return, marks the systolic pressure.
The ABI is defined as the ratio of the higher brachial pressure to each of the ankle pressures. A ratio of around 1 is considered normal, while lower values indicate various levels of significant peripheral arterial disease (PAD) according to international guidelines.
Doppler Measurments
Peripheral vascular Doppler measurements are normally performed using CW (Continuous Wave) Doppler probes.
Different Probe frequencies are used depending on the target vessels: 4 or 8 MHz are used for larger and deeper vessels such as the Carotid, Femoral or Popliteal arteries, and higher 8 or 10 MHz are used for the smaller and shallower vessels such as the Dorsalis Pedis or Tibial arteries.
The main objective is to qualitatively examine the waveform shapes: a normal peripheral artery (not in the carotids) will show 3 phases during a cardiac cycle, a prominent early systolic forward flow, a late systolic reverse flow, followed by a small component of forward flow again. This signifies a healthy elastic artery. As the vessel becomes less elastic (for example due to diabetes), the third and/or second phase will disappear.
In addition, significantly high velocities may indicate the presence of a stenosis or some other obstruction to the blood flow.
Pulse Volume Recording
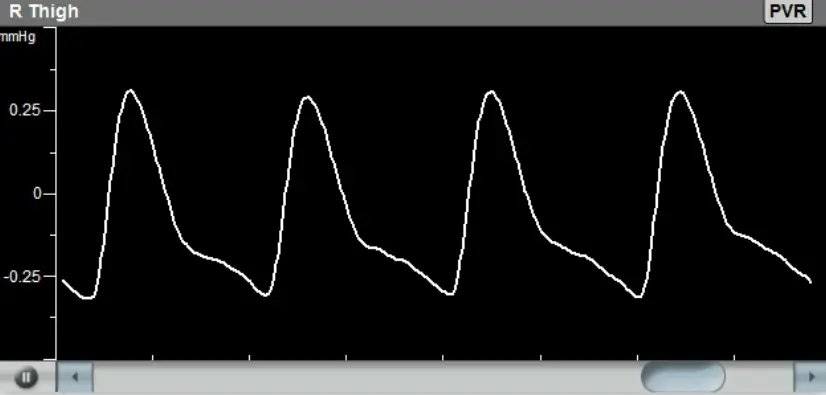
The Pulse Volume Recording (PVR) test is a pneumo-plethysmographic test used for detection of the segmental volume changes in the limb which result from the flowing blood, as a function of the cardiac cycle.
Similar to the Segmental Blood Pressure (SBP) measurements, dedicated pressure cuffs are placed around all limb segments prior to initiating the test.
The cuffs are then inflated to a pressure that would occlude the venous return, yet will maintain the arterial flow un-obstructed. This pressure is typically 65 mmHg.
Once the cuff pressure is stabilized, the waveform signals which reflect the segmental volume changes can be recorded. The clinicians are normally interested in the qualitative shape of the waveforms: a “normal” PVR consists of a rapid systolic upstroke and a rapid downstroke with a prominent dicrotic notch.
With increasing arterial disease the PVR waveform becomes attenuated, the upstrokes and downstrokes are less prominent and the PVR amplitude decreases and ultimately becomes flat.
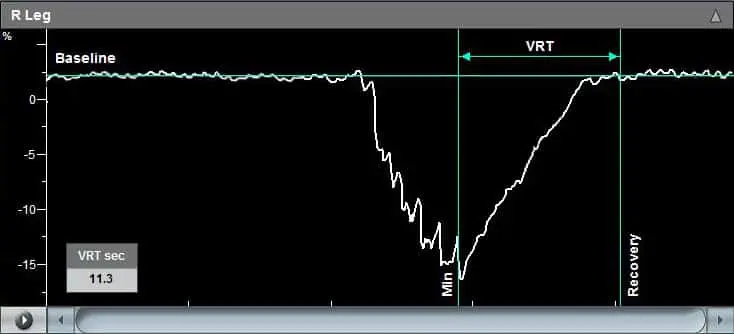
Venous Reflux
The Venous Reflux test is used to determine the competence of the superficial venous valves in the calves of the legs. This test is performed with a DC PPG sensor.
When performing Venous Reflux test, the patient is requested to sit upright with the legs not touching the ground. A Photo-plethysmograph (PPG) sensor is attached to the leg above the ankle in the region of the posterior tibial artery. When the DC signal reaches a steady state baseline, the patient is requested to perform multiple leg dorsiflexions which result in “pumping” of all of the venous blood. After the dorsiflexions the patient is requested to remain still, while the PPG DC signal returns back to the initial baseline.
Optionally, the test can be repeated with a cuff wrapped around a segment on the leg (thigh, above/below knee) acting as a tourniquet.
The duration from the end of the dorsiflexions (maximal signal change) until the signal return to baseline (VRT, Venous Recovery Time) indicates the status of the valves. A slow recovery time indicates competent valves, while a fast VRT would indicate a suspicion of valvular incompetency.
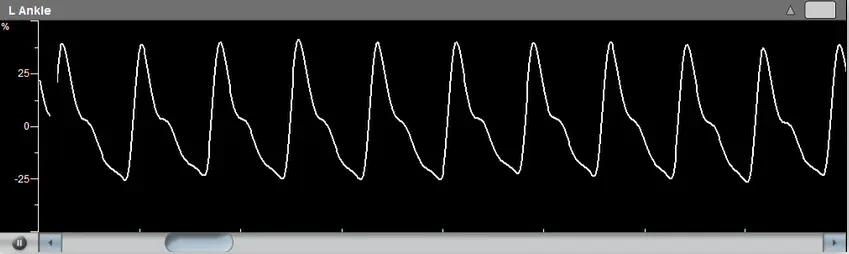
PPG Readings
The Photo-plethysmograph (PPG) test detects changes in segmental blood volume, in a similar manner to the Pulse Volume Recording (PVR) test. The PPG technology, however, is different than the pressure-sensor based PVR technology.
With PPG, infra-red signals are transmitted to the skin and reflected back to the sensor, therefore PPG waveforms reflect local and rather shallow skin variations in blood flow.
Typical PPG measurement sites are the toes and digits, and interpretation of the signals is in a similar manner to the interpretation of the PVR waveforms.


Exercise Stress Test
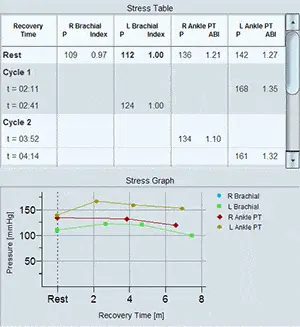
Segmental pressures are often measured at different post-stress times to determine also the recovery time from the stress effects. The clinician is particularly interested in identifying significant variants from the resting pressure indices and specifically changes in the Ankle-to-Brachial Index (ABI).
On the left side is an example of a Segmental Blood Pressure measurement with induced stress (exercise in this case) performed using Viasonix FALCON/Pro. The table shows blood pressure measurements in pre-exercise and post-exercise conditions. It is common to take multiple measurements (cycles) in timed intervals after performing the induced stress. The stress graph on the left side shows the recovery of each measured segment starting with pre-stress conditions until the last post-stress cycle.
In order to differentiate different vascular disorders, or to determine the functional severity of a stenosis, some of the tests described above are repeated after induced stress.
Typically, the patient will be requested to perform treadmill or similar activity, under the supervision of the examiner.
Most of the time the stress testing will include Segmental Blood Pressures, particularly at the ankles and brachials, and sometimes also Pulse Volume Recording (PVR) and CW Doppler measurements.

Theracic Outlet Syndrome
The Thoracic Outlet Syndrome test is conducted in order to determine the vascular role when the patient’s symptoms are indicative of perfusion loss or neurogenic causes.
This procedure tests for intermittent perfusion loss, particularly in the arms and hands.
Either Doppler, PVR or PPG sensors detect normal resting waveforms in the digits or hands and then the patient is instructed through a sequence of positions such as: Hands-up Test, Adson or Scalene Maneuver, Costoclavicular Maneuver, Allen Test, and Provocative Elevation Test.
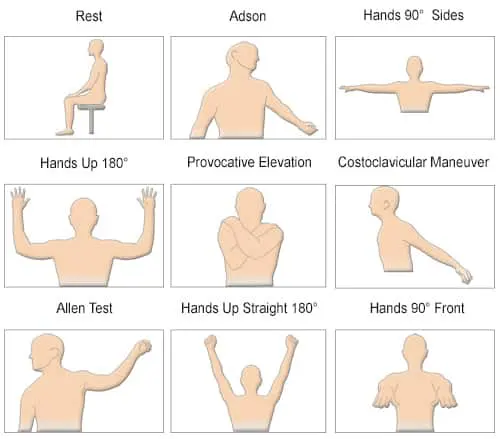
The clinician tries to identify a position which significantly reduces perfusion to determine whether the symptoms originate from vascular causes.
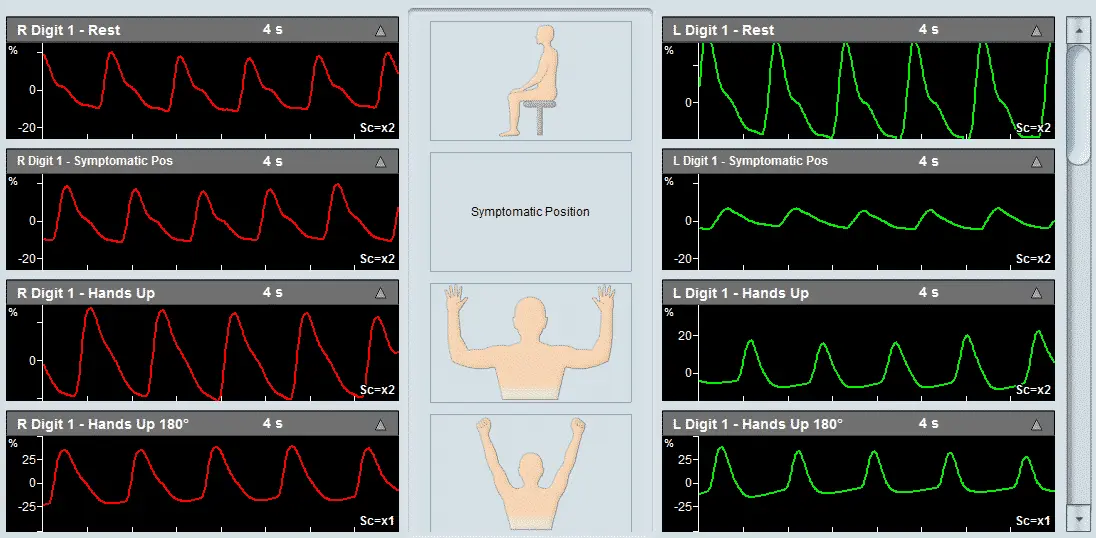
Raynaud's Syndrome
The Thoracic Outlet Syndrome test is conducted in order to determine the vascular role when the patient’s symptoms are indicative of perfusion loss or neurogenic causes.
This procedure tests for intermittent perfusion loss, particularly in the arms and hands.
Either Doppler, PVR or PPG sensors detect normal resting waveforms in the digits or hands and then the patient is instructed through a sequence of positions such as: Hands-up Test, Adson or Scalene Maneuver, Costoclavicular Maneuver, Allen Test, and Provocative Elevation Test.
MVO/SVC Determination
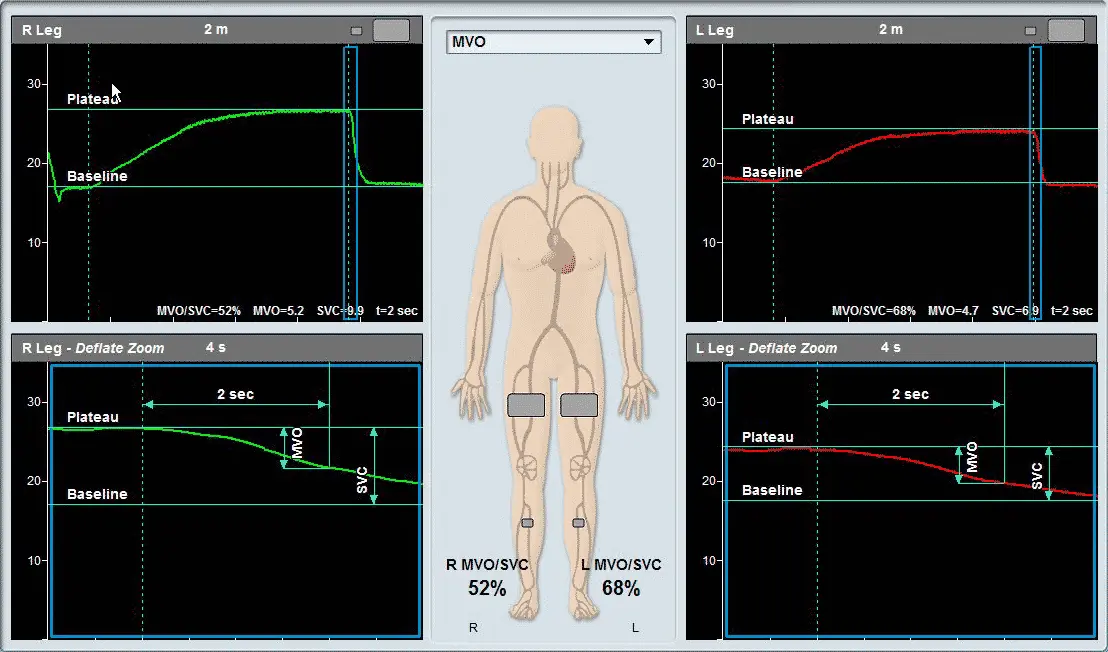
The MVO/SVC test determines the Maximum Venous Outflow (MVO) and the Segmental Venous Capacitance (SVC).
The patient lies in a supine position with the legs slightly elevated. A venous occluding cuff is placed on the thigh and a Pulse Volume Recording (PVR) pressure cuff is placed on the calve.
Initially, the sensor (PVR or PPG) is measured and a baseline is determined. Then the thigh cuff is inflated to occlude the venous return (around 60 mmHg) and the changes in the sensor signal are recorded. Once a plateau is reached, the occluding cuff is rapidly deflated. The sensor signal also quickly returns back to the initial baseline. The clinician then determines MVO and SVC based on the sensor signal to determine venous functionality.
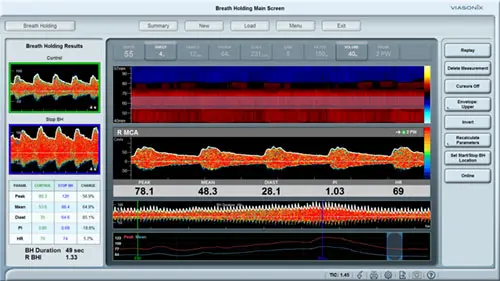
Reactive Hyperemia
The Reactive Hyperemia test is allowed only in certain countries.
Stress testing is frequently used in peripheral vascular diagnosis to differentiate between different vascular disorders, or to determine the functional severity of an arterial stenosis. Systolic pressures are measured before and after inducing vascular stress. While typically the patient is asked to perform a physical exercise such as exercise on a treadmill, sometimes the patients have difficulties in performing exercise.
In special cases, the reactive hyperemia test (RH) can replace the standard exercise tests and induce vascular stress. RH requires to inflate a pressure cuff in order to occlude the blood flow to the limb or segment of interest for up to several minutes, and then rapidly releasing the cuff pressure in order to generate the hyperemic effect.
It is crucial that a professional examiner will be present near the patient at all time, and immediately deflate the pressure cuffs when necessary.
Penile Function
Penile function or impotence test is used for determination of whether penile function disorders are of vascular nature.
The Viasonix FALCON/Pro allows to use a variety of tests, including the simultaneous combination of different tests. Such tests include Doppler arterial measurements in the penile vessels, blood pressure measurements with a penile pressure cuff, and PVR or PPG waveform measurements.
The results of such tests can either identify a penile vascular problem, or eliminate vascular issues as the cause of impotence.
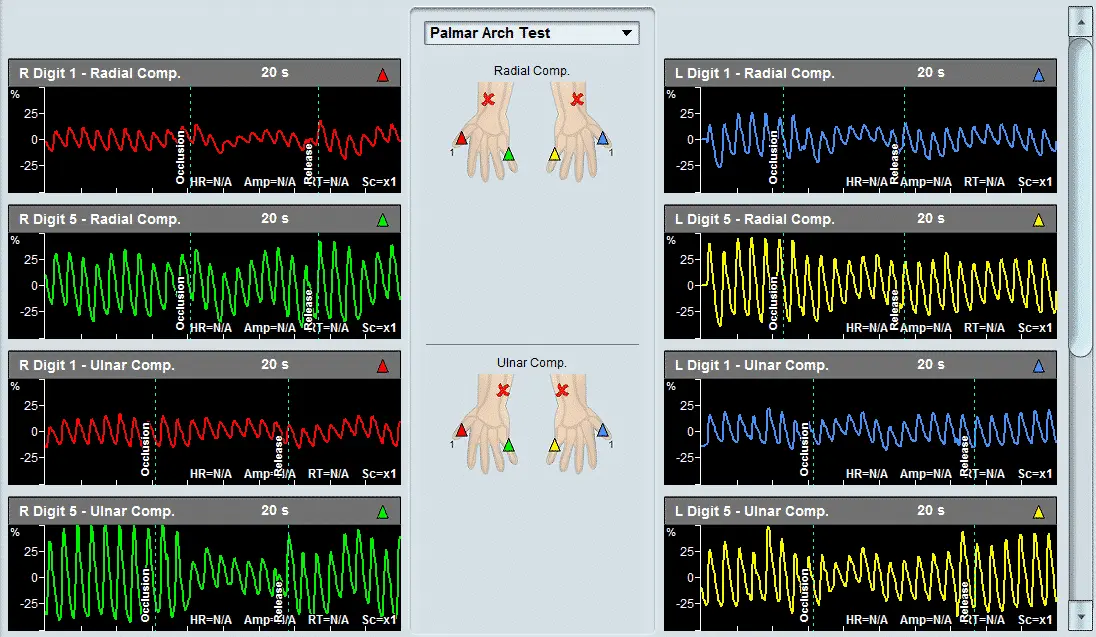
Palmar Arch Test
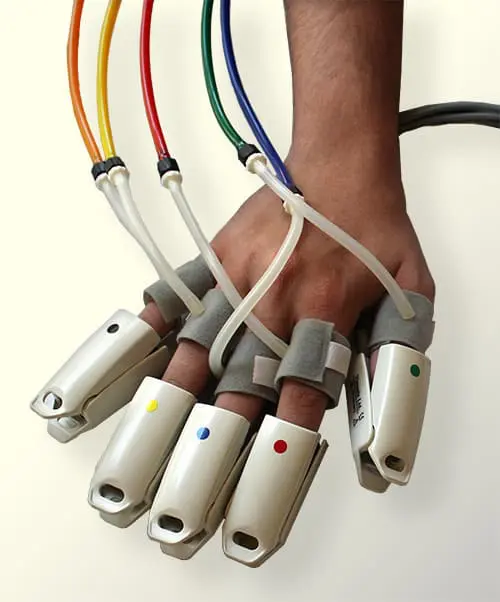
The Palmar Arch Test (PAT) is a specialty test performed to evaluate the patency of the Palmar arch in the hand prior to radial or ulnar artery harvesting in artery bypass procedures or before the surgical creation of an upper extremity hemodialysis fistula or graft.
Typically, 2 PPG sensors (photo-plethysmograph) are placed on the two extreme digits (digit 1 and digit 5). The FALCON/Pro allows placing even 5 PPG sensors on all five digits. The Palmar Arch Test protocol begins by measuring the resting PPG waveforms, then measuring the waveforms after selected compressions (compression of the radial artery, ulnar artery, or both) and finally measuring the waveforms after the release of the selected compression.
Compression is typically performed by manually compressing the selected artery or arteries. This procedure allows the examiner to evaluate whether the compression results in impeded or loss of blood flow to parts of the hand. Thus, significant reduction or loss of blood flow to areas of the hand suggests that removing that particular artery may jeopardize hand performance if the artery is removed.
Clear markers in the waveforms indicate when artery compression begins, and when the compression is released.