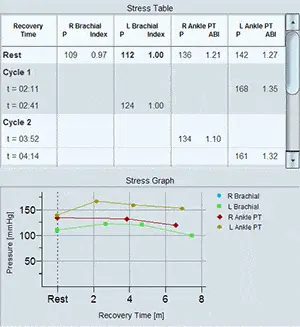
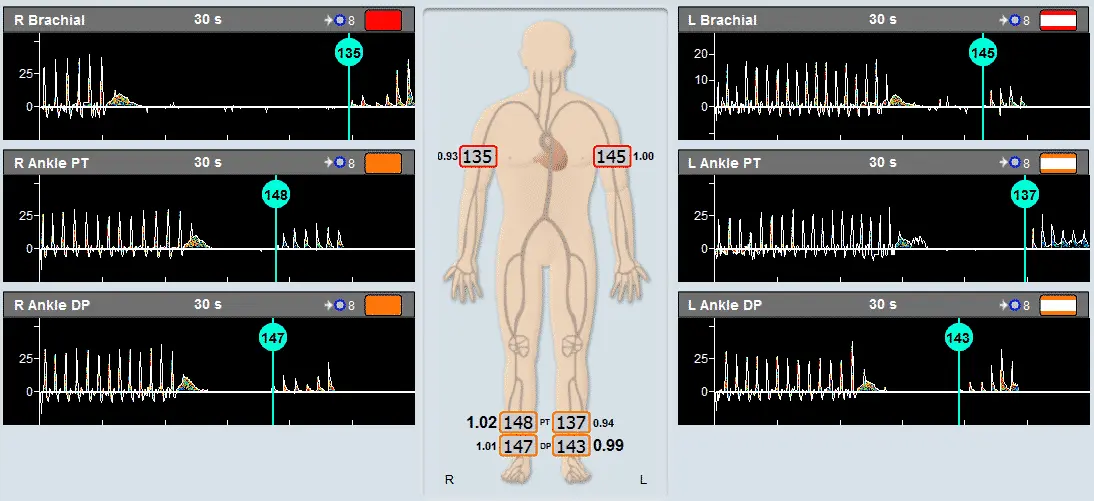
ABI, the Ankle Brachial Index, is the most popular application for fast and simple screening of a physiological vascular pathology. With this test pressure cuffs are placed on the 2 ankles and on 1 or 2 brachial segments.
The Viasonix FALCON Pro allows to perform the ABI test with either Doppler or PPG sensors. In addition, the Falcon allows to perform simultaneous measurements in all sites under certain conditions for rapid measurements.
Prior to segmental cuff inflation, a reference signal is identified distal to the cuff location. When the cuff pressure exceeds the systolic pressure, the reference signal waveforms should disappear. Then, the cuff pressure is slowly deflated at constant bleeding rate, and the first occurrence, of the reference signal waveform return, marks the systolic pressure.
The ABI is defined as the ratio of the higher brachial pressure to each of the ankle pressures. A ratio of around 1 is considered normal, while lower values indicate various levels of significant peripheral arterial disease (PAD) according to international guidelines.