Peripheral arterial disease (PAD) is a common disease in Western societies. The most common symptom of PAD is intermittent claudication. When PAD becomes more severe, the affected limb can develop rest pain, ulceration, and gangrene. In some cases, it may even require minor or major amputation. Timely diagnosis and revascularization may save a patient’s limb. As PAD is part of systemic atherosclerosis, early diagnosis of PAD may help detect the presence of atherosclerosis. This may result in early intervention including cardiovascular risk stratification and risk factor modification.
PAD diagnostic guidelines recommend clinical assessment and diagnostic testing. Clinical evaluation is essential which includes the clinical history, review of symptoms, and physical examinations. A patient with PAD may have one or more of the following physical examination findings:
- abnormal lower limb pulse,
- vascular bruit,
- nonhealing lower limb wound,
- lower limb gangrene and other suggestive signs of lower limb ischaemia.
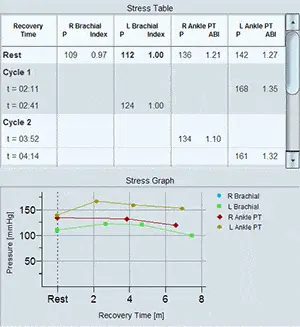
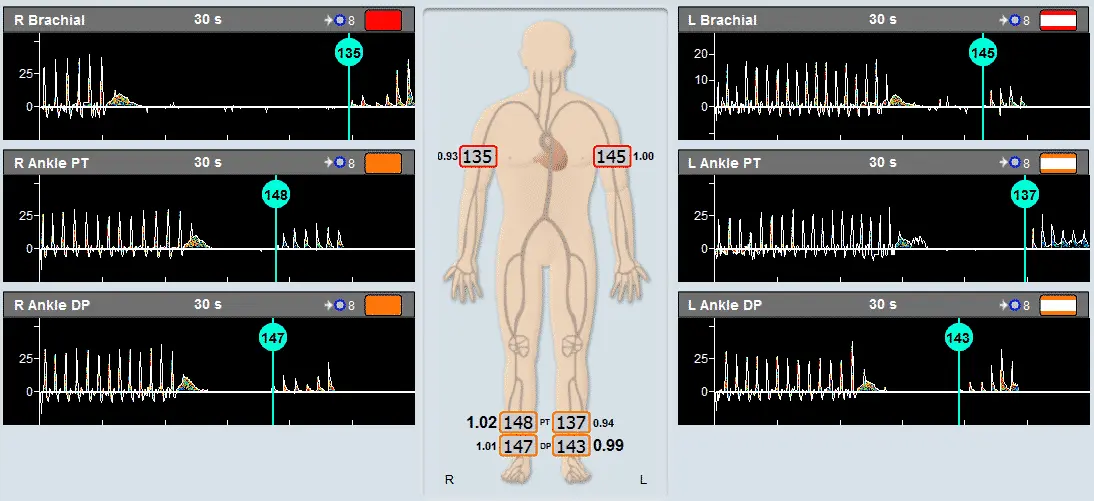
Guidelines recommend to apply diagnostic testing to confirm clinical suspicion of PAD. The resting ankle-brachial index (ABI) is the initial diagnostic test for PAD. The resting ABI is a simple, non-invasive test that is performed by measuring systolic blood pressure in the arms (brachial arteries) and ankles (dorsalis pedis and posterior tibial arteries) using a vascular diagnostic system. The ABI of each leg is calculated by dividing the higher of the dorsalis pedis pressure or posterior tibial pressure by the higher of the right or left arm blood pressure (Figure 1).

Figure 1. Resting ABI test using Doppler method.
Based on clinical presentation and the resting results, additional physiological testing may be required. Treadmill exercise ABI testing can objectively measure functional limitations attributable to lower limb symptoms and is especially useful in establishing the diagnosis of lower limb PAD in the symptomatic patient with normal or borderline resting ABIs. The toe-brachial index is used to establish the diagnosis of PAD in the setting of incompressible ankle arteries, and to assess perfusion in patients with suspected critical limb ischaemia.
Anatomical imaging studies such as duplex ultrasound, computed tomography angiography, magnetic resonance angiography, or digital subtraction angiography may be performed if clinically indicated. These tests are usually carried out when patients are considered to receive interventional or surgical revascularization.
While it is not universally agreed, there are practice guidelines which recommend screening for PAD in patients with high risk of atherosclerosis, presence of exertional leg pain, age >65 years old, and age >50 years old who either smoke or have diabetes. The most commonly used PAD screening test is resting ABI. The ABI values between 1.0-1.4 are considered as normal, 0.9-0.99 as borderline PAD, <0.9 as diagnostic of PAD, and >1.4 suggests non-compressible ankle arteries. Early detection of asymptomatic PAD may identify patients with increased risk of cardiovascular events and mortality. Initiating secondary prevention of cardiovascular disease may reduce their risk.
The ABI test is the diagnostic test of choice for diagnosis and screening of PAD. Melbourne based MedTech Edge supplies Viasonix Falcon, an all-in-one vascular physiological diagnostic system which is capable of performing the ABI test and many other vascular tests for peripheral arterial and venous disease (Figure 2).

Figure 2. Viasonix Falcon Pro vascular diagnostic system.